In Montana’s 147,000 square miles of frontier, geography isn’t just a backdrop, it’s a defining force that shapes healthcare access and outcomes. Harsh weather and considerable distances to premier care centers make accessing cancer treatment especially difficult for rural residents. Travel is often unpredictable and unsafe, given that 76% of Montana’s roads remain unpaved, and the state is home to 290 mountain passes that are regularly impacted by snow and ice.
A study utilizing 5 years of cumulative data (2014-2018) from the Montana Tumor Registry assessed the impact of geographic disparity on cancer care for patients in Montana and found that 19.2% of state residents did not receive treatment following a cancer diagnosis; the highest percentages were observed in counties distant from Commission on Cancer (CoC)-approved centers. The analysis indicated that the distance from these centers was the single most significant factor in lack of treatment, more so than socioeconomic status and lack of insurance.
A Community Facing Multiple Barriers to Care
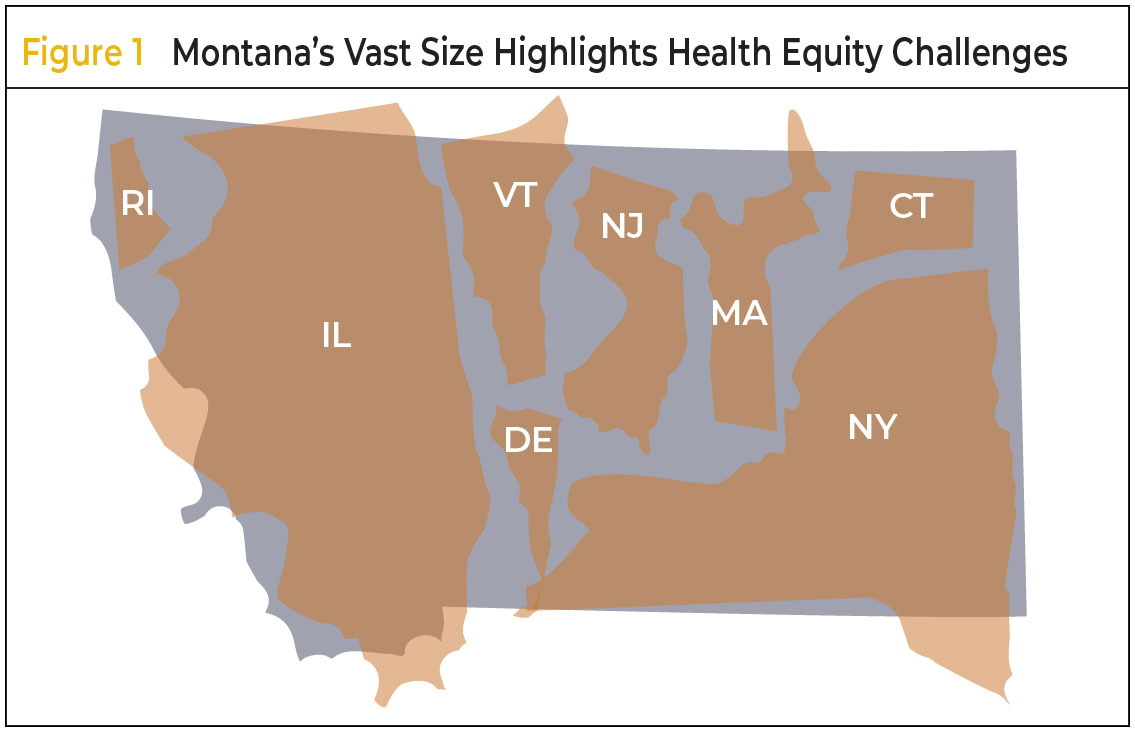
Montana, although sparsely populated, spans a landmass large enough to contain multiple eastern states, posing unique challenges for health equity (Figure 1).
Dillon, a town of approximately 4000 residents in southwest Montana, epitomizes the challenges faced by the area’s rural communities. The nearest regional cancer center is 130 miles away, and the nearest federally designated cancer center is 360 miles away—distances that become insurmountable during severe weather. At Barrett Hospital and HealthCare, the local critical access hospital, chemotherapy infusions were not offered, meaning many patients had no option but to travel up to 6 hours for treatment—or go without.
Compounding these geographic challenges were workforce shortages. Recruiting trained oncology providers to critical access hospitals—smaller facilities designated to serve rural populations—is difficult, particularly when existing infrastructure can’t support comprehensive cancer care services. As a result, patients not only lacked local access to chemotherapy but also had limited access to diagnostic consultations and survivorship care.
Building a Better Model Through the Alliance
The Alliance for Equity in Cancer Care is a national, 5-year initiative focused on improving access to high-quality oncology services for underserved populations. As part of the Alliance, ASCO and its affiliate, Conquer Cancer, The ASCO Foundation, are supporting efforts in Montana to decrease the geographic barrier to cancer care.
The Alliance has enabled ASCO to partner with Barrett Hospital and HealthCare and Bozeman Health Cancer Center to bring oncology services to this frontier region of the state. Bozeman Health, a regional CoC cancer center 115 miles northeast of Dillon, was already equipped with a full suite of cancer care services.
Rather than employing a traditional “hub-and-spoke model”—which can reinforce hierarchical relationships between institutions—Barrett Hospital and Bozeman Health adopted a collaborative cancer care delivery model grounded in shared governance, mutual investment, and joint service development while respecting the independence of each institution. This partnership offers more than just clinical support; it provides a blueprint for transforming rural healthcare delivery.
Designating Dillon as a Pilot Site
Dillon emerged as the ideal pilot site thanks to a unique convergence of community readiness and infrastructural opportunity. Bozeman Health already had an established clinical relationship with Barrett Hospital through prior outreach visits from Bozeman Health oncologists, which laid the foundation of trust and familiarity. This was coupled with catalyst financial support from the Alliance that helped facilitate the coordination of a collaborative cancer infusion center. Primary care providers in the Dillon area were queried to assess their receptiveness to a new care delivery model, as primary care providers are the primary referrers to cancer care. Responses were positive and emphasized a need for access to high-quality services.
Leadership at both healthcare centers also expressed substantial interest in building a dedicated oncology service line, and several key elements were already in place: pharmacy infrastructure capable of safely preparing chemotherapy, an active outpatient infusion service line, and local staff committed to expanding capacity. Critically, the CEOs of both institutions demonstrated strong support for the project, recognizing its long-term value for the community. Financial modeling further confirmed the initiative’s viability by projecting the patient volume and resources needed to support sustainable operations. This solid foundation and preparation positioned Barrett Hospital to move from concept to implementation in less than 2 years.
Launching Local Cancer Care
The partnership culminated in the creation of the Oncology Clinic and Infusion Center at Barrett Hospital in October 2024, offering local chemotherapy, oncology consultations, and survivorship care. To support the expansion, Barrett Hospital invested in facility upgrades, including clinical space renovations to accommodate infusion chairs, exam rooms, and provider offices. Then, installation of the Beacon Oncology Module within the EPIC electronic medical record system enabled seamless clinical coordination. Finally, the initiative emphasized workforce development. To support the center, a number of staff have received training, including hands-on learning at Bozeman Health, and pursuit of national certifications through the Oncology Nursing Society and Hematology/Oncology Pharmacy Association. A multidisciplinary team—comprising an advanced practice provider, registered nurses, a clinical pharmacist, and medical assistants—was cross-trained to deliver high-quality, locally managed oncology care.
The approach strengthens both institutions. Bozeman Health is able to expand its reach and serve more patients without overextending its resources, while Barrett Hospital gains the capacity to deliver high-quality oncology care—and eventually other services—close to home. Even more importantly, it enhances cancer care for patients in need. To date, patients have been able to receive both treatment and follow-up care totaling more than 265 total visits, saving an estimated 64,000 miles in travel and $13,650 in attributable fuel costs alone. Furthermore, travel burden was reduced by 1060 hours of drive time, which could conservatively translate to more than $28,600 in increased income (based on the Montana average wage of $27.00/hour).
“It has been extremely rewarding to see the impact this program has had on our patients and community. Witnessing a patient ring the bell at the conclusion of her chemotherapy, when previously she would have chosen hospice instead of burdening her family with traveling for cancer care, has certainly been a highlight,” said Sarah Adsit, PA-C, a physician assistant at Barrett Hospital.
Beyond Oncology: A Blueprint for Rural Care
ASCO highlights 3 pillars of implementation success: alignment, leadership commitment, and strategic catalyst funding (Figure 2). In partnership with Montana State University, data collection and evaluation of the collaborative model is underway.
The success of this model demonstrates the power of community-driven, cross-institutional collaboration to expand access to specialty care in rural and frontier areas. Plus, the approach offers a replicable framework for other rural institutions seeking to expand specialty care access in geographically isolated regions. The partnership also provides a roadmap for extending similar collaborations across other specialties, such as cardiology or behavioral health, with the potential to transform rural health ecosystems more broadly.
As health systems across the United States seek to increase access to cancer care, the Dillon model offers a compelling way forward. By centering community input and mutual investment rather than relying on top-down systems, institutions can create durable service lines that increase access, enhance local capacity, and improve outcomes. In doing so, lifesaving oncology care has already been brought home to one Montana community—offering a model that could benefit many more across the rural United States.
The collaborative cancer care delivery model in Montana has profoundly transformed patient access, demonstrating that geographical distance is no longer an insurmountable barrier to high-quality treatment.
These invaluable lessons learned from this innovative, partner-led approach are now poised for dissemination, offering a blueprint for accessible high-quality oncology care across similar rural and frontier landscapes.
Source
- Hensold JO, Zimmerman H, Merrill JK, et al. The impact of geography on receipt of cancer treatment in Montana. J Clin Oncol. 2022;40(suppl). Abstract 140.
Copyright © 2025 Journal of Oncology Navigation & Survivorship. Reprinted with permission.
Three Lessons From Conquer Cancer, the ASCO Foundation
- Shared Vision & Aligned Goals: Successfully launching new initiatives, especially in complex healthcare environments, hinges on all stakeholders not just understanding but truly sharing a unified vision and ensuring their individual goals are fully aligned with the overarching objective.
- Strong Leadership Buy-In: Consistent, visible commitment and active support from leadership at all levels are indispensable. Their advocacy helps secure necessary resources, navigate bureaucratic hurdles, and instill confidence and motivation across the implementing teams.
- Strategic Catalyst Funding: Initial, dedicated “catalyst” dollars are critical for overcoming the financial barriers often faced by new programs, particularly in rural settings. This up-front investment provides the essential runway for infrastructure enhancements, staffing and training, and operational stability until long-term sustainability can be established.